HOW TO MAKE A DIAGNOSIS OF URETHRAL STENOSIS?
The diagnosis is made through a series of investigations.
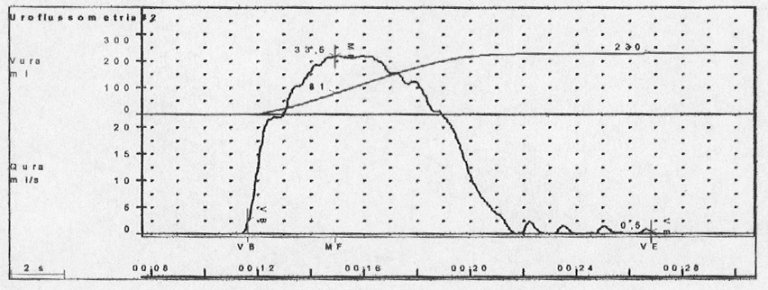
a. Uroflowmetry
The urine pressure is measured during the voiding phase with the use of a container, as if one were going to the bathroom. If the reduction in flow strength reaches a (maximum flow <12 ml / sec.), it may indicate an obstacle to urination and therefore the presence of a stricture.
b. Urethrography
This is a radiological examination with a contrast medium that visualizes the urethra and bladder.
This exam is divided into two phases:
 1. Retrograde urethrography
1. Retrograde urethrography
A small catheter is placed inside the external urethral meatus (only a few centimeters) and the contrast medium is injected, through the catheter, into the urethra, so as to visualize the urethral canal. The examination does not require any preparation, but must be carried out with the close collaboration of the patient who must, for a few minutes, bear the discomfort of the catheter in the penis and of the contrast medium that flows along the urethra.

2. Voiding urethrography
Once the bladder is filled with the contrast agent, introduced into the urethra retrograde, the patient will have the sensation of maximum filling of the bladder. The catheter is removed and the patient is invited to urinate. X-rays are taken during the voiding phase.
c. Urethroscopy
Urethroscopy is an endourological procedure that allows the exploration of the urethra internally with special instruments, semi-rigid and flexible. The urethroscope is connected to a camera that allows the urologist to see on the monitor the urethra internally (the appearance of the mucosa, the presence of neoformations, the presence of stones).
Other additional exams include:
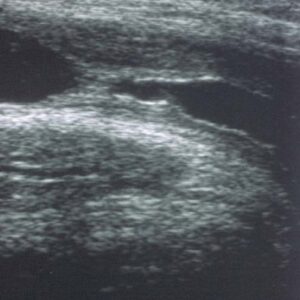
Ultrasound of the urethra
This is an investigation that gives additional information: the exact length of the diseased urethral tissues involved in the urethral stricture.
Urine culture
In the presence of urethral strictures the culture is often positive due to the complete emptying of the bladder.
How to resolve URETHRAL STENOSIS?
Surgery is required to resolve urethral stenosis. The choice of surgery depends on the characteristics of the urethral stricture (cause, length and location) and the patient’s history (age, related diseases, general conditions, etc.)
There are two types of surgery on the urethra:
- Endoscopic urethrotomy
- Urethroplasty
Endoscopic urethrotomy
Urethrotomy refers to the endoscopic treatment of the narrowing of the urethral canal.
The purpose is the incision and opening of the narrow urethral canal, thus allowing a good urination. The technique consists of one endoscopic incision of the urethral canal using a “cold blade” and can be performed blind (urethrotomy according to Otis) or under vision (urethrotomy according to Sachse). For some years the internal urethrotomy has also been performed using a laser.
Duration of the procedure: the operation usually lasts a few minutes and can be performed either in general anesthesia or with a simple sedation of the patient.
Duration of admission: after the operation a bladder catheter is left in situ. In the absence of complications the hospital stay is only one night.
URETHROPLASTY
Urethroplasty consists of surgical repair of the urethral canal. In relation to the characteristics of the lesion (length, cause of stenosis, fistula or presence of urethral calculi) and to local tissue conditions, the surgeon reserves the right, during the operation, to choose the surgical solution from a range of different techniques more suitable.
All urethroplasty, except the termino-terminal anastomosis, foresees the possibility of having to resort to the use of tissue transplants without their own vascular support (grafts) or with a vascular support (flaps). The grafts are generally of skin taken from the prepuce or from other extragenital skin regions, or of mucosa generally taken from the inside of the cheek or lip. The flaps, on the other hand, are skin areas with their own vascular peduncle. All surgical interventions on the urethra provide the possibility of performing histological examination of a sample of the urethra in order to highlight pathologies that require further treatment or careful monitoring over time.
A. SINGLE-TIME URETHROPLASTY
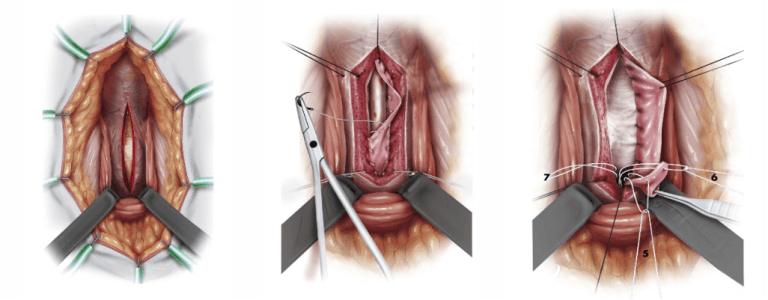
Termino-terminal anastomosis
Consists in dissecting at full thickness the diseased urethral tract, removal of the fibro-sclerotic tissue and reunification of the two urethral stumps. With this intervention the urethra is repaired with a single intervention.
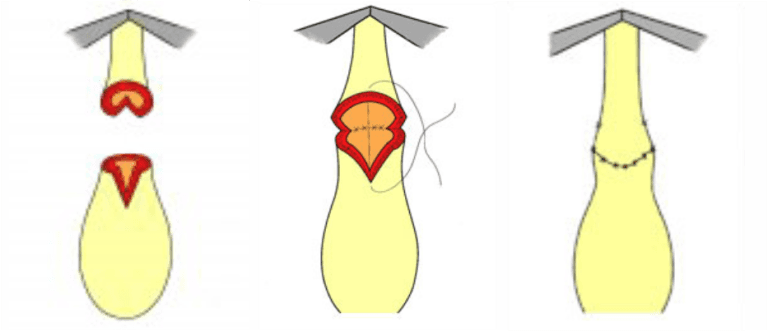
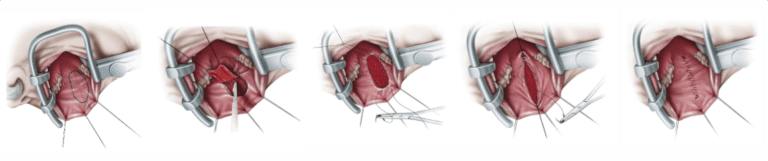
Enlargement urethroplasty of the urethral lumen using transplants of skin or mucous tissue.
The urethra is opened longitudinally at the level of the stenotic tract and the canal is enlarged with a strip of oral mucosa, taken from the inside of the cheek or from the tongue. It is a real self-transplant, as the mucous membrane is completely detached from the inside of the mouth or from the tongue and sutured on the urethra with various techniques ( urethroplasty with dorsal, ventral or double graft graft..)
Buccal mucosa (MB)
The buccal mucosa is currently the first choice of tissue to be used in urethral surgery.
The use of the buccal mucosa has replaced the use of the penile skin which is not always well accepted by the patient because it requires circumcision.
The sample is taken from the inner cheek and the wound is sutured: the discomfort in the mouth lasts only a few days, the patient can resume eating the day after the operation and the stitches are reabsorbed spontaneously after about 1 month. It is not advisable to take a lip extraction because there is a risk of complications: difficulty opening the mouth, altering the expression of the face.
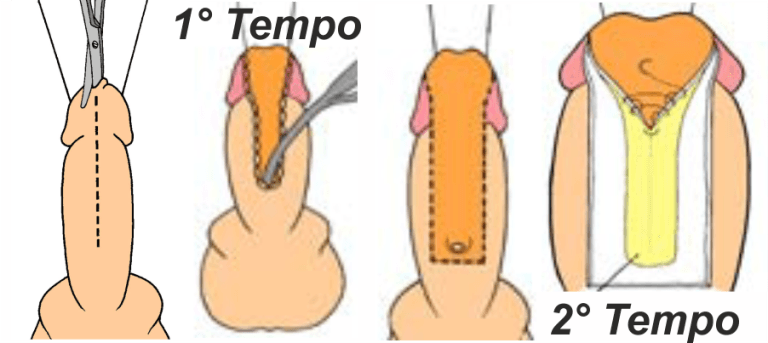
B. URETHROPLASTY IN TWO STAGES
The urethra is repaired with two or more operations, carried out over a time span of 6 to 12 months.
In stenosis of the penile urethra, during the first operation, the urethra is opened or completely removed and replaced by a wide strip of oral mucosa or skin of the penis, which is sutured directly on the cavernous bodies and on the glans. If the graft is well vascularized, the mucous membrane is transformed into a tube and the urethra is returned to the center of the glans after about 6-12 months.
1st stage:
This consists of the opening of the urethral canal, the formation of a new urinary meatus at the level of the perineum or along the ventral surface of the penis (penile urethrostomy) depending on the length of the stenosis.
2nd stage:
This consists of the surgical closure of the aforementioned urinary deviation (perineal or penile uretrostomy) with consequent reconstruction of the continuity of the urethral lumen. In the end, therefore, the patient returns to urinate from the original urinary meatus.
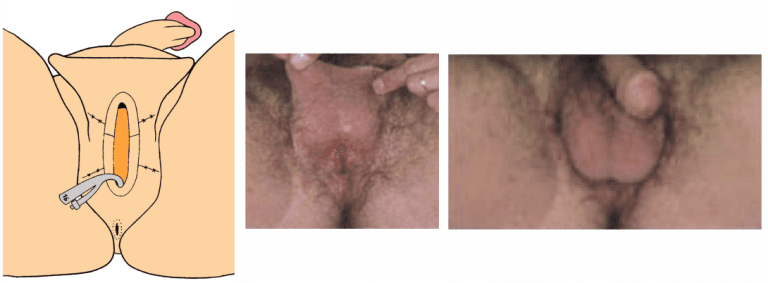
In stenosis of the bulbar urethra, during the first operation, the urethra is opened under the scrotum and the urine comes out of this new ostomy, forcing the patient to urinate in a sitting position. When possible, this perineal stoma can be closed again, allowing the patient to urinate again through the penis. In other cases, perineostomy is definitive, as urination through the penis cannot be restored to the patient.
In the interval between the 1st and 2nd time of a two-stage urethroplasty it may be necessary to resort to surgical revision of the urethra due to the progression of the basic urethral stenosing pathology. These revisions may correspond from the surgical point of view to actual uretroplastics.